If alexithymia were a fixed biological trait, prevalence rates would be roughly the same everywhere. They are not.
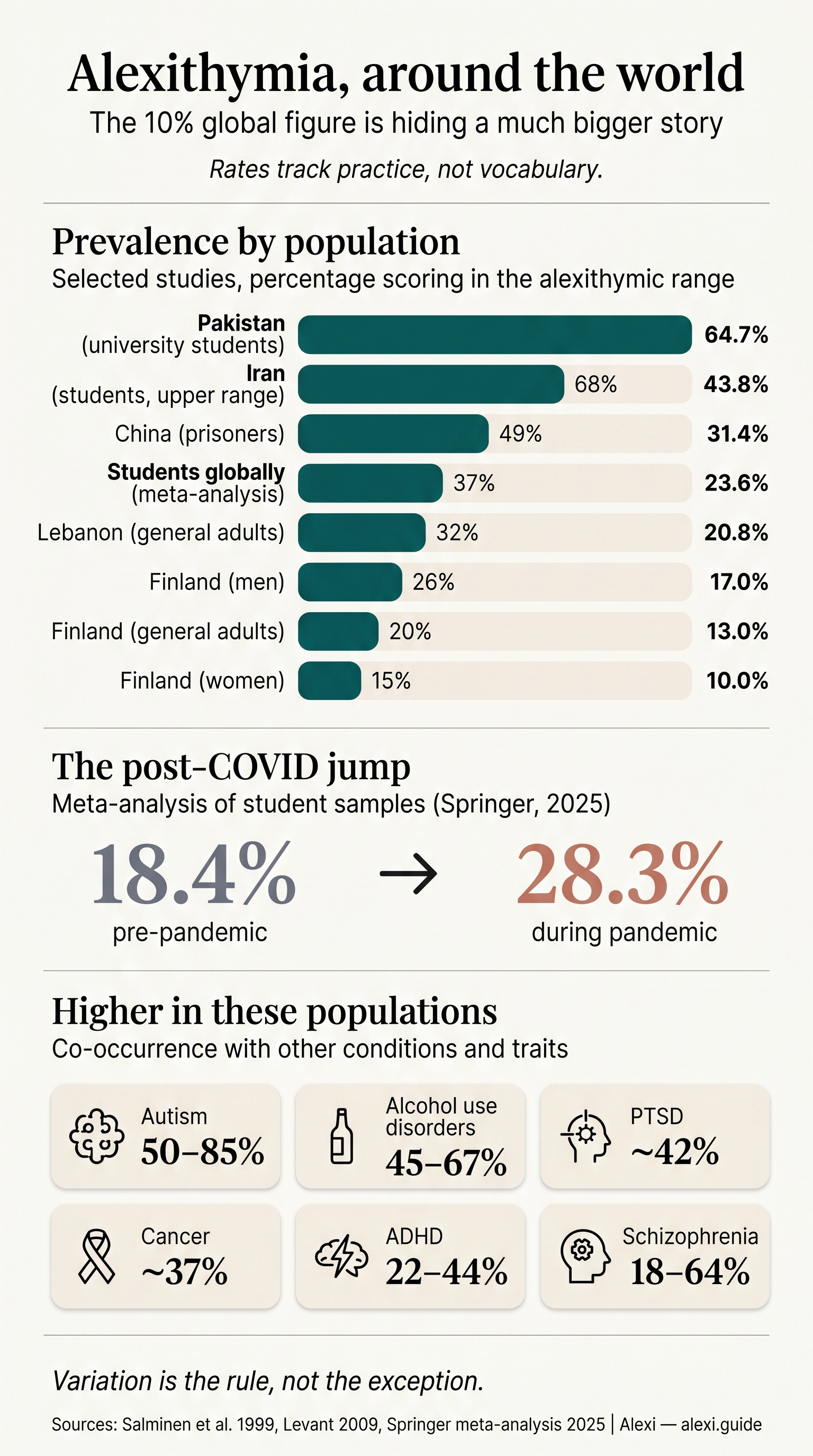
In Finland, the most-cited general-population study puts the figure at 13%. In Iran, university-student samples have come back at 21.8% in one city and 43.8% in another. In a 2021 sample of medical students in Riyadh, more than half scored either definite or possible alexithymia prevalence on the Toronto Alexithymia Scale. In a Karachi medical-student sample, the rate hit 64.7%. These are not measurement glitches. The instrument behaves consistently across cultures. The numbers themselves are doing the talking.
What follows is a worldwide tour of what the peer-reviewed literature actually says about alexithymia prevalence — where it is high, where it is low, and why the rates vary so much. This article is informational, not a diagnosis. If you arrived here looking for a definition first, the pillar explainer covers the trait in full. The piece below assumes you already have the gist: alexithymia is a difficulty identifying and describing what you feel, treated by current research as a trait — like introversion — rather than a disorder. Roughly one in ten people, on the most conservative read.
But “one in ten” is a rounded average pulled from a single Finnish dataset. The reality is far more interesting, and far more useful if you’re trying to work out whether the trait is wired into you or partly inherited from the language and gender norms you grew up inside.
The “10% global” figure is hiding a much bigger story
Almost every consumer-facing article on alexithymia cites the same number: 10% of the population. Some round to “around one in ten.” A few are honest enough to write 8–13%. The figure comes from a 1999 paper by Salminen and colleagues, who surveyed 1,285 adults in Finland using the 20-item Toronto Alexithymia Scale, the TAS-20. It is still the standard instrument used in almost every prevalence study you will see referenced.
The Salminen paper is good. It is also one country, one decade, one instrument, one cut-off score. Treating its 13% as a global constant is the central error of consumer alexithymia coverage, including the high-DR pages that currently dominate the search results.
When you actually look at the cross-cultural literature on alexithymia worldwide, the picture fractures. Asian-heritage samples score consistently higher than European-heritage samples. Middle Eastern student samples sit two to four times higher than the Finnish baseline. Post-COVID student samples jumped roughly ten percentage points in a single meta-analysis. Men score higher than women in nearly every general-population study, but not in every clinical sample.
The TAS-20 is not the problem. Cross-cultural validation work, including the Perth Alexithymia Questionnaire’s measurement-invariance studies between Iranian and American respondents, suggests the construct itself travels. The variation in alexithymia prevalence is real. Something other than biology is producing it.
Finland, where the modern numbers come from
The Salminen study deserves a closer look, because almost everything else in this article is calibrated against it.
In 1999, Salminen, Saarijärvi, Äärelä, Toikka and Kauhanen published prevalence figures for 1,285 Finnish adults: 13% overall, 17% in men, 10% in women. The sample was broadly representative of the Finnish working-age population. They used the TAS-20 with the standard cut-off, and ran multivariate analyses to identify what predicted a positive screen. Four variables came out: male gender, advanced age, low educational level, and low socioeconomic status.
A subsequent Finnish paper put adolescent prevalence at 7.3%, lower than the adult rate, with girls slightly higher than boys at younger ages and the relationship inverting later. Young Finnish adults sat at 9.4% for men and 5.2% for women.
Alexithymia in Finland matters not because Finns are unusually alexithymic but because Finland produced the most defensible early general-population dataset, and the country has remained a methodological reference point. When you read “the prevalence of alexithymia is around 10%”, you are usually reading a soft echo of Salminen 1999. The figure is real for Finland, in the 1990s, in a population with a particular history of emotional reserve. It is not a global average. It was never meant to be.
Why Asian samples consistently score higher than European samples
Pull together every TAS-20 study comparing Asian-heritage samples with European-heritage samples and one pattern shows up over and over: the Asian sample scores higher. The gap is not subtle, and it is not random.
The cross-cultural team led by Andrew Ryder, with Catherine Dere, Yulia Chentsova-Dutton and Iris Sunohara, has spent years working out why. Their answer, in short: the difference is not biology. It is emotion-socialisation. Cultures along what gets loosely called the Confucian axis — China, Japan, Korea, and the broader East Asian region they have shaped — train children from early childhood to regulate emotional expression rather than narrate it. The norm is reserve, not articulation. Outward emotional disclosure, especially of negative affect, can be read as immature, indulgent, or socially burdensome.
The TAS-20 captures three sub-factors: difficulty identifying feelings (DIF), difficulty describing feelings (DDF), and externally-oriented thinking (EOT). When researchers decompose the cross-cultural gap by sub-factor, most of the East-Asian difference loads onto EOT, the tendency to think about external events rather than internal states. That is exactly what you would predict if the rate difference is being driven by socialised emotional restraint rather than wired-in interoceptive deficit.
The construct itself, importantly, holds up. The Perth Alexithymia Questionnaire’s psychometric work shows the same five-factor structure across Singaporean, Australian, Iranian and American samples. The instrument is measuring the same thing everywhere. The cultures it is measuring it in are different.
China, Japan, and the Confucian shadow
Specific Chinese samples make the pattern concrete. Alexithymia in China is one of the most-studied non-Western variants of the trait, partly because Chinese researchers have been validating and reporting TAS-20 data steadily since the early 2000s. A 2017 study of adult prisoners in China, published in BMC Psychiatry, found a TAS-20 alexithymia rate of 31.4% — roughly two and a half times the Finnish general-population baseline. Hong Kong adolescent samples have come back elevated, with researchers explicitly linking the gap to Confucian emotional-restraint norms. Chinese HIV/AIDS patients show elevated rates. Mainland Chinese adolescents with depression studied during the pandemic in Anhui Province scored 76.45%, versus a roughly 26.75% pre-pandemic baseline in the same clinical population.
Alexithymia in Japan is harder to pin down because the Japanese-language TAS-20 work is less synthesised in English-language literature, but cross-cultural comparisons including Japanese male samples consistently place them above European baselines. The framing in Japan, as in China, treats emotional restraint as a virtue rather than a deficit. A man who does not narrate his feelings is, in many social contexts, not failing. He is performing competence.
This is the crucial reframe. A 31.4% rate in Chinese prisoners and a 13% rate in Finnish adults are not measuring two different prevalences of the same biological trait. They are measuring two different blends: a small wired-in core, plus a much larger learned dialect of emotional expression that varies enormously by where you grew up and how the adults around you handled their own feelings.
If you have East Asian heritage and you score high on a TAS-20, you are not necessarily more alexithymic in the trait sense than a Finn who scored 20 points lower. You may be more fluent in restraint and less fluent in narration. The two are not the same.
Iran, Saudi Arabia, and the rest of the Middle East
The highest documented rates in the literature come not from East Asia but from the Middle East and South Asia, in student and medical-student samples.
In Iran, university-student samples range from 21.8% at Babol University of Medical Sciences to 43.8% at Shahrekord University of Medical Sciences (2019–2020 academic year, n=290). In Saudi Arabia, a 2021 cross-sectional study of 420 medical students at King Saud University in Riyadh found 26.9% definite alexithymia plus a further 24.3% scoring “possible” — a combined caseload above 50% in a population of high-achieving young adults. A prior Saudi study in Jeddah reported 49%. Lebanese student samples sit at around 20.8%. Jordanian samples come in at 24.6%. A Karachi medical-student sample produced 64.7%, the highest single figure in the recent peer-reviewed literature. Tunisia, by contrast, came in at 16.5%, closer to the European range.
Three factors plausibly account for the cluster. First, gendered emotional norms. Boys in much of the region are socialised toward stoicism, reinforced by religious and cultural codes that treat emotional articulacy as feminine or weak. Second, trauma exposure. Several of the highest-prevalence countries have endured prolonged conflict, displacement, or political instability. Secondary alexithymia, the trait emerging as a response to chronic stress, is a recognised pattern. Third, sample bias: medical students and university students worldwide score higher than general-population adults. The post-COVID meta-analysis discussed below puts the global student average at 23.6% across 17 studies. Comparing a Saudi medical cohort to a Finnish general-population cohort is not quite comparing like with like.
One Saudi finding cuts against the global pattern: women in the Riyadh sample scored slightly higher on the TAS-20 than men, with a mean of 54.84 versus 51.43 (p=0.006). The global default is the reverse. This is a useful reminder that the men-higher pattern is not universal. It is the modal finding in Western samples, not a biological constant.
Comparing the numbers: alexithymia prevalence by country
Most consumer pages quote a single number. Here is the cross-cultural picture in a single table — alexithymia statistics gathered from the studies referenced above. Treat it as a starting map, not the last word. The populations are not all directly comparable, and the article notes underneath the table matter.
| Country / region | Population studied | Prevalence | Year / source |
|---|---|---|---|
| Finland | General adults (n=1,285) | 13% (men 17%, women 10%) | Salminen et al., 1999 |
| Finland | Adolescents | 7.3% | Honkalampi et al. |
| Finland | Young adults | Men 9.4%, women 5.2% | Mattila et al. |
| Tunisia | Medical students | 16.5% | Cross-sectional |
| Lebanon | General / mixed | 20.8% | Regional comparison |
| Iran (Babol) | University students | 21.8% | Babol UMS |
| University students globally | Meta-analysis, 17 studies (n=11,603) | 23.6% | Multi-country pooled |
| Jordan | General / mixed | 24.6% | Regional comparison |
| Saudi Arabia (Riyadh) | Medical students (n=420) | 26.9% definite + 24.3% possible | KSU, 2021 |
| Students worldwide, post-COVID | Meta-analysis | 28.3% (vs 18.4% pre-COVID) | Springer, 2025 |
| China | Adult prisoners | 31.4% | BMC Psychiatry, 2017 |
| Iran (Shahrekord) | Medical students (n=290) | 43.8% | Shahrekord UMS, 2019–20 |
| Saudi Arabia (Jeddah, prior) | Medical students | 49% | Earlier KAU study |
| Pakistan (Karachi) | Medical students | 64.7% | Karachi cross-sectional |
| China (Anhui, COVID-era) | Adolescents with depression | 76.45% | Multi-hospital, 2020–21 |
The standard instrument across nearly all these studies is the TAS-20, with the standard cut-off score. Rates from different population types — general adults, students, prisoners, depressed clinical samples — are not directly comparable, and the table makes that obvious. What it shows is range: roughly five to one between the lowest defensible general-population figure and the highest student-cohort figure, and considerably wider once you include depressed clinical samples.
The English-speaking countries: why we don’t have great UK or Australian numbers
If you live in the UK, Australia, Ireland, or New Zealand and you are looking for a national alexithymia prevalence figure, you will not find one. There is no Salminen-equivalent for any of them. This is a real gap, and it is itself a finding.
The UK literature relies heavily on autism-overlap proxies. Autistica, the UK’s main autism research charity, has a short alexithymia explainer focused on autistic adults. PTSD UK covers the trauma-overlap angle. Estimates of alexithymia in autistic adults sit at 50–85% co-occurrence, which gives you a defensible upper bound for the autistic UK population but says nothing about the general adult population. Australia has small psychiatric-versus-community comparison studies published in journals like Psychiatry Research, plus some autism-framed work from Reframing Autism, but again no general-population epidemiology.
The honest answer for a UK or Australian reader is: extrapolate cautiously from Finland, expect the figure to be of similar order of magnitude given broadly similar individualist emotion-socialisation, and treat any national point-estimate you see floated for these countries with scepticism. The data does not yet exist.
That gap is part of why this project is written in British and Australian spelling. The literature is thin and the consumer coverage is overwhelmingly American. The local picture deserves better.
Men vs women: the “normative male alexithymia” pattern
Across most general-population studies, men score higher than women on alexithymia measures. Salminen’s Finnish data put the male rate at 17% and the female rate at 10%, close to a two-to-one gap. A 2024 meta-analysis on gender differences in alexithymia produced a Cohen’s d of 0.22, a small effect, with men higher.
The most useful framing of this gap comes from Ronald Levant, the American psychologist who in the 1990s coined normative male alexithymia. The argument: in many cultures, boys are socialised out of emotional articulacy. Crying is shamed, vulnerability is mocked, the emotional vocabulary that girls absorb in childhood is actively pruned in boys. The result is a learned dialect of restraint that, on a TAS-20, looks indistinguishable from the trait itself.
The TAS-20 sub-factor breakdown supports this read. Men consistently score higher on Difficulty Describing Feelings (DDF) and Externally Oriented Thinking (EOT), but not on Difficulty Identifying Feelings (DIF). In Salminen’s data, men and women were essentially equal on DIF. Men felt their feelings as well as women did. They were less practised at putting them into words.
This matters globally because it means the gender gap is not biology. It is a learned dialect. If you are a man who scored high on a TAS-20 and you live in a country where masculine emotional reserve is rewarded, your score is partly measuring a trait and partly measuring your fluency in your culture’s gendered emotional grammar. For partners trying to make sense of this from the outside, the field guide to loving someone with alexithymia goes deeper.
The post-COVID rise (and why students were hit hardest)
A 2025 systematic review and meta-analysis in Current Addiction Reports (Springer) pooled cross-sectional studies of alexithymia in students and produced two pooled prevalence figures: roughly 18.4% before the COVID-19 pandemic and 28.3% during or after it. A roughly ten-percentage-point absolute increase, in the same population type, in the same kind of study, in the space of about three years.
The Chinese clinical data is even starker. In depressed adolescents, the rate moved from a pre-pandemic baseline of around 26.75% to 76.45% in the 2020–2021 Anhui Province sample. Three times higher in the same clinical group.
What changed? The Springer authors point to the obvious candidates: prolonged isolation, the collapse of unstructured peer interaction at exactly the age developmental psychologists believe emotional vocabulary is shaped, screen-mediated relationships replacing embodied ones, and chronic background stress. None of these are biological in any deep sense. They are environmental factors that, on the trait-not-disorder reading, would be expected to increase secondary alexithymia without changing the underlying primary-trait base rate.
Whether the rise is permanent is genuinely an open question. A cohort whose adolescence was spent indoors, socialising through a screen, may carry the effect into adulthood. Or the dialect may catch up once the developmental scaffolding returns. The literature is not yet old enough to tell.
What this means if you suspect alexithymia in yourself
The strongest thing you can take from a worldwide tour of prevalence data is this: a meaningful share of what looks like alexithymia in any individual person is learned dialect rather than fixed wiring.
If you grew up in a culture, family or gender role that rewarded restraint and punished emotional narration, your TAS-20 score is partly measuring a trait and partly measuring an inheritance. The trait part — the wired-in core, what the literature sometimes calls primary alexithymia — does not really go away. The dialect part is teachable, slowly, with patience. Most people who do this work describe it less as fixing themselves and more as picking up a second language late.
That distinction matters because it changes what kind of intervention makes sense. It is not therapy in the heroic sense. It is vocabulary-building, body-attention, and the small daily practice of noticing what is happening in you before you decide what to call it. The pillar explainer covers the trait itself in detail, and the practical guide to building an emotional vocabulary covers the work. Both assume you already have the relief of a name for it. That is usually the first move.
FAQ
Is alexithymia more common in any specific country?
Yes, the prevalence of alexithymia varies substantially by country. The lowest defensible general-population figures come from Finland (around 13%) and similar Northern European samples. The highest documented rates come from Middle Eastern and South Asian student and medical-student samples — Iran (21.8–43.8%), Saudi Arabia (combined definite-plus-possible above 50% in one Riyadh sample), and Pakistan (64.7% in a Karachi medical-student sample). These rates are not directly comparable because the populations differ (general adults vs students vs clinical samples), but the underlying variation is real and is mediated by emotion-socialisation norms, gender expectations, and trauma exposure rather than biology.
Why do men have higher rates of alexithymia than women?
In most general-population studies men score higher than women. Finland’s Salminen study put the gap at 17% versus 10%, and a 2024 meta-analysis estimated a Cohen’s d of 0.22. The pattern is concentrated on the “describing feelings” and “externally-oriented thinking” subscales of the TAS-20, not on “identifying feelings” — meaning men feel their feelings about as well as women do but are less practised at narrating them. The American psychologist Ronald Levant calls this normative male alexithymia: the result of growing up in cultures that socialise boys out of emotional articulacy. The gap is gendered socialisation, not innate biology.
Did COVID actually make alexithymia worse?
The peer-reviewed evidence so far points to yes, particularly in students. A 2025 Springer meta-analysis pooling cross-sectional studies estimated that pre-pandemic student prevalence was around 18.4% and rose to roughly 28.3% during or after the pandemic — a ten-percentage-point absolute increase. In a Chinese sample of adolescents already living with depression, the alexithymia rate moved from about 26.75% pre-pandemic to 76.45% in 2020–2021. The likely drivers are isolation, disrupted peer interaction during a developmentally sensitive period, and screen-mediated relationships replacing embodied ones. Whether the rise is permanent is not yet known.
Are Asian people really more alexithymic, or is the test biased?
Cross-cultural psychometric work suggests the TAS-20 and the Perth Alexithymia Questionnaire measure the same construct across cultures. The test is not the problem. The higher Asian rates are real, but the right interpretation is not “more emotionally deficient.” The cross-cultural research team led by Andrew Ryder, Catherine Dere, Yulia Chentsova-Dutton and Iris Sunohara argues the gap reflects emotion-socialisation: collectivist and Confucian-influenced cultures train children toward emotional restraint and externally-oriented thinking rather than internal narration. The trait core may be roughly equal; the learned dialect is different.
Does language affect alexithymia rates?
There is no strong evidence that the structural richness of a language’s emotion vocabulary directly drives prevalence rates. Finnish, Mandarin and Arabic are not lacking words for feelings. What does seem to matter is how much practice the language gets — whether parents, teachers and peers actually model emotional narration, whether describing how you feel is socially normal or coded as childish or self-indulgent, and whether the gendered codes around emotional disclosure are rigid or loose. Rates track practice, not vocabulary.
We publish the Emotional Colourblindness guide for those living with alexithymia and the people who love them. Read more →