You came here trying to work out which one you have. Or which one your partner has. Or — if you’ve already been diagnosed with one — why the others keep showing up in your search history.
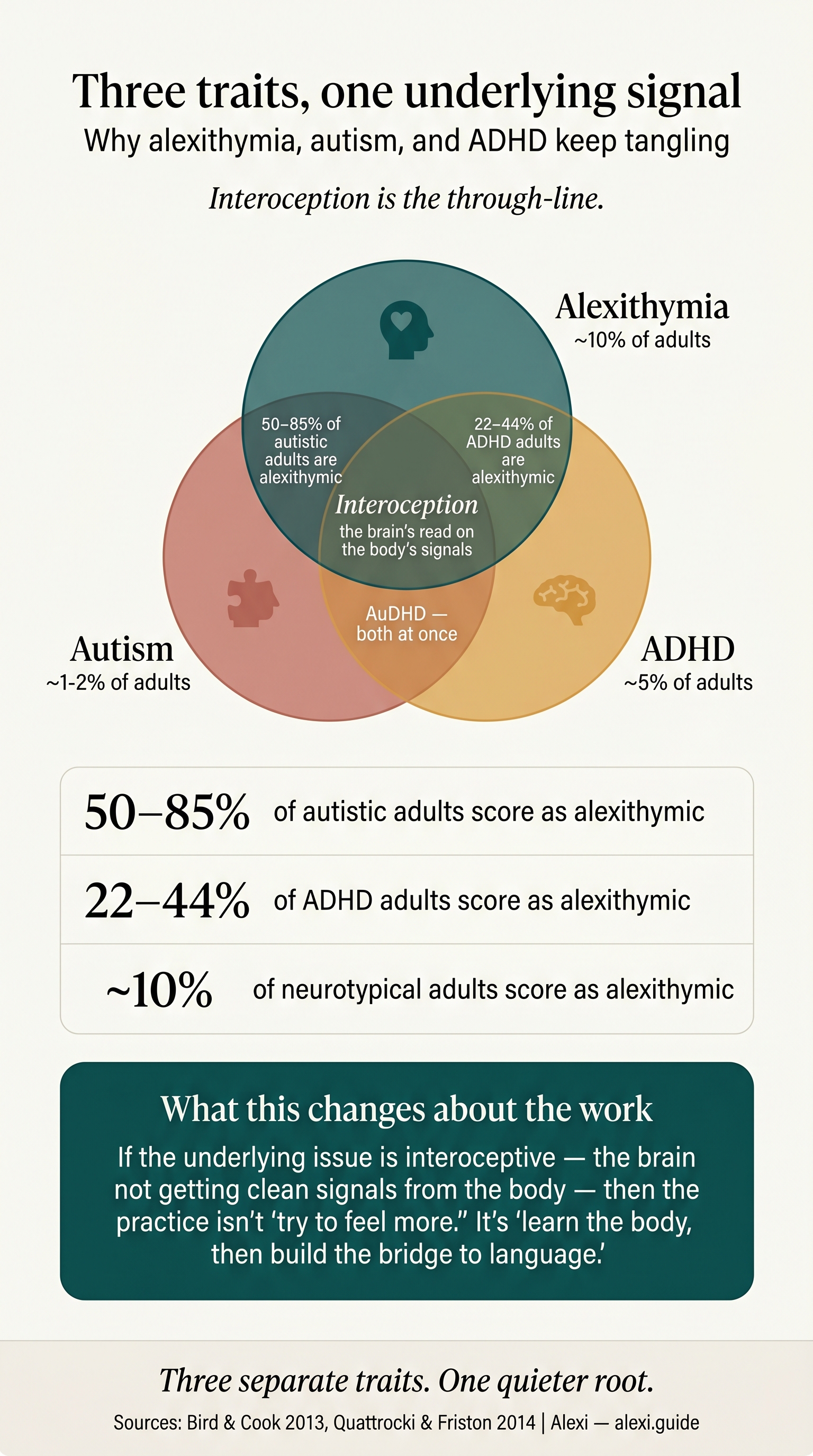
There is a reason these three keep tangling. The relationship between alexithymia and autism is the most-cited overlap in the neurodivergent literature, with roughly half to four-fifths of autistic adults scoring in the alexithymic range. ADHD sits a step behind, with somewhere between a fifth and nearly half. AuDHD — the both-and population — stacks the odds further. None of which means alexithymia is autism, or autism is alexithymia. They are three separate traits that happen to share a quieter, deeper root: the way the brain reads signals from the body. That is what this piece is about.
A note before we go further. Alexithymia is a trait, not a disorder — like introversion. Autism is a neurodevelopmental difference. ADHD is a difference in attention regulation. This article is informational, not a diagnosis; the foundational definitions live in the pillar guide on alexithymia. If a section here lands in a way that feels destabilising rather than clarifying, please pause. Lifeline (AU) 13 11 14, Samaritans (UK) 116 123, 988 (US/CA).
The numbers: how alexithymic the neurodivergent population actually is
The figures are striking enough that they often get cited without context, so here they are with the context.
Autism. Across the published literature, somewhere between 50% and 85% of autistic adults score above the threshold for alexithymia on the Toronto Alexithymia Scale (TAS-20). The wide range reflects different samples and different cut-offs; a frequently-cited synthesis puts it at 49.93–85%, against 4.89–13% in the general adult population. Whichever end of that range you trust, the autistic population is roughly five to seven times more likely to be alexithymic than the general one.
ADHD. The ADHD figures sit lower but still well above baseline. Edel and colleagues, in a 2010 sample of 73 adults with ADHD, found 22% scored above the alexithymia threshold and reported substantially higher social anxiety than the non-alexithymic ADHD group. A decade later Kiraz, Sertçelik and Erdoğan Taycan (2021) studied 100 adult ADHDers and found 41.5% — a near-doubling, and one with a clear link to impulsivity. The honest range to quote is 22–44%.
General population. Roughly one in ten adults — 13% in Salminen and colleagues’ Finnish general-population sample, with men closer to 17% and women closer to 10%.
AuDHD. The data are thinner because AuDHD as a clinical framing only became common in the last few years. Both populations are independently elevated; both share the underlying mechanism we’ll come to. If your wiring is both, the chance you also experience alexithymia goes up, not down.
Why these three keep getting mistaken for each other
A reader doing late-night research often arrives with a list of symptoms and three plausible labels. The reason they keep blurring is that all three can present with the same outward sign — a person who looks unreadable, undemonstrative, or fine — for genuinely different underlying reasons.
ADHD’s version is time-blindness and delayed processing. The feeling is happening; you just don’t notice it until later, sometimes much later, sometimes only when your body forces the issue. To a partner asking what’s wrong in real time, the honest answer is nothing I can find yet. That looks like emotional flatness. It isn’t.
Autism’s version is monotropic attention — the tendency to focus deeply on one stream of input at a time. If your attention is locked on a problem, a conversation, or a sensory texture, the affect channel can simply not register on your face. You’re feeling something; it just isn’t being broadcast.
Alexithymia’s version is the one this guide is about: the emotion is happening, the body is registering it, and the bridge from sensation to language has not been built. The signal arrives and dies on the way to the word. The three can stack — and in AuDHD with alexithymia, all three mechanisms can be running in the same person at the same moment. Which is why a single label rarely tells the whole story.
What alexithymia is, what autism is, what ADHD is — in three plain-English paragraphs
Alexithymia is a trait, present in roughly 10% of the general population, characterised by difficulty identifying your own emotions, difficulty describing them, and a tendency to focus outward when asked how you feel. The full definition — including the three sub-factors used by the TAS-20 (DIF, DDF, EOT) and the Type I / Type II distinction — is laid out in the pillar guide. For our purposes: when someone asks how do you feel, the honest answer is I don’t know, and the not-knowing is genuine, not evasive.
Autism is a neurodevelopmental difference shaping how a person processes sensory input, social signals, and patterns of attention. It is not a disorder of empathy, and it is not a personality. Autistic people tend to perceive detail more sharply, transition between contexts less smoothly, and read social signals through a different — often slower, more analytical — channel than non-autistic people. The framing here is difference, not deficit.
ADHD is a difference in attention regulation, often described as an interest-based or salience-based attention system rather than an importance-based one. The brain attends to what is novel, urgent, or emotionally engaging — and struggles to attend to what is merely important. It comes with documented differences in dopamine signalling, executive function, and emotional reactivity.
These three traits are independent. You can have any one without the others. They co-occur at higher-than-chance rates, but the correlation does not collapse the categories.
The autism overlap, in detail
The autism-alexithymia overlap is the tightest and the most-studied, and the one most likely to surprise readers who arrived here assuming the two were interchangeable. They aren’t. The reason they look interchangeable is a piece of research that quietly rearranged the field.
In 2013, Geoff Bird and Jennifer Cook published what is now called the alexithymia hypothesis: the proposal that several emotional features long attributed to autism — difficulty recognising emotions in others, blunted empathic responses, atypical processing of facial expression — actually correlate with alexithymia rather than with autism per se. In a separate 2013 study, Cook, Brewer, Shah and Bird showed that poor recognition of facial emotion in autistic samples disappeared once alexithymia was controlled for. The participants could see the physical structure of the face perfectly well; what they struggled with was the emotional interpretation. The trait doing the work, in other words, was alexithymia, not autism.
Berthoz and Hill (2005) found that autistic alexithymia tends to be the cognitive type rather than the affective type — difficulty identifying, verbalising, and analysing emotion, rather than experiencing it. Which fits what autistic alexithymics consistently report: the feeling is in the body, sometimes intensely so, and the gap is between body and word.
This matters for two reasons. First, alexithymia in autistic adults is not autism in disguise; it is a separate trait riding alongside, accountable for a chunk of what looks like the emotional dimension of autism. Second, you can address one without the other. Working on alexithymia — building the bridge from interoceptive signal to language — is not the same project as working on autism, and it does not require an autism diagnosis to begin.
A note on alexithymia in autistic women. The picture is under-studied because autistic women are under-diagnosed. Masking — the conscious effort to perform neurotypical affect — can hide alexithymic blankness behind a learned smile or a rehearsed sentence. The result is a person who reads as fine, sometimes for decades, and who privately has no idea what she feels.
The ADHD overlap, in detail
ADHD comes with its own canonical emotional feature: ADHD emotional dysregulation. The fast surge, the rejection-sensitive flare, the meltdown that arrives in 90 seconds and is gone in three. That is not alexithymia. Alexithymia is the inverse — emotion that should be there and isn’t quite getting through. The two can stack, and the stacking is what produces the curious lived experience of I feel everything and nothing at once.
The numbers, recapped: Edel and colleagues (2010) found 22% of 73 adult ADHDers scored above the alexithymia threshold; the alexithymic subgroup also reported markedly higher social anxiety. Kiraz and colleagues (2021) found 41.5% in a sample of 100, and demonstrated a clear correlation with trait impulsivity — the alexithymic ADHDers were more likely to act on emotion they could not yet name.
The mechanism, in plain terms: ADHD emotions surge faster than the identification system can catch up. By the time you’ve got a word for it, you’ve already snapped, withdrawn, eaten the thing, sent the text. ADHD time-blindness compounds this; the present-tense awareness that should let you say I’m getting overwhelmed often only kicks in retrospectively. I felt fine until I didn’t is a sentence almost every adult ADHDer has spoken.
Alexithymia adds a second floor to that building: even in retrospect, even with time, the word doesn’t come. You know something happened. You can’t tell anyone what it was. The result is an emotional life that feels both turbulent and inarticulate — and is often misread by partners, by therapists, by the person living it.
The AuDHD reality (and why most clinical pages ignore it)
If you’re quietly recognising both columns — autism and ADHD — you are not unusual, and you are not making it up. The both-and population is real, increasingly well-documented, and almost entirely absent from the older clinical literature, where autism and ADHD were until recently treated as mutually exclusive diagnoses.
AuDHD means the autistic monotropic focus and the ADHD novelty-driven attention shift are running in the same nervous system. They contradict each other constantly. You hyperfocus, then crash. You need routine, and routine bores you. You shut down at sensory overload, then seek stimulation an hour later. Add alexithymia and the whole thing becomes harder to narrate from the inside, because every state has multiple plausible causes, and the body signal that would normally let you sort them isn’t reliably reaching language.
The practical implication is liberation, oddly. If you’ve spent years trying to assign every blank, every shutdown, every misfire to a single cause — was that the ADHD, or the autism, or the alexithymia, or just being tired? — you can stop. The honest answer is often all three, in some proportion, and the body knows even if the word doesn’t. Naming the AuDHD-with-alexithymia pattern is not a diagnostic act. It is a permission to stop demanding a tidier story than your nervous system supplies.
Interoception is the through-line
This is the section that pays for the article. Once you see it, the autism-ADHD-alexithymia tangle stops looking like a Venn diagram and starts looking like three branches of the same root system.
Interoception is the internal sense of bodily state — your perception of your heart rate, your breath, your gut, your temperature, the tension in your jaw, the tightness in your chest. It is the channel through which the body tells the brain what is happening to it. Most current emotion theory treats interoception as the substrate of feeling: an emotion is, at minimum, the brain’s interpretation of an interoceptive pattern in context.
In 2014, Quattrocki and Friston published an influential paper proposing that alexithymia is fundamentally an interoceptive predictive coding problem. In their model, the alexithymic brain is not getting clean signals about bodily state — or is getting them and not weighting them properly — so the raw material that emotion-naming depends on simply isn’t there in usable form. Subsequent work by Hayley Murphy, Caroline Catmur and Geoff Bird has reinforced the picture: interoceptive accuracy and alexithymia are tightly linked, and the link holds independent of autism. Alexithymia is its own trait; the interoceptive substrate is what underlies it.
Now drop autism and ADHD into the picture. Both come with documented interoceptive differences. Autistic individuals show altered interoceptive accuracy in multiple studies, with implications ranging from delayed hunger recognition to atypical pain processing. ADHD interoceptive research is younger but converging: differences in heartbeat detection, in body-state attention, in the integration of internal signal with present-moment awareness. The reason alexithymia rates are so elevated in both populations is not coincidence. All three traits sit on top of an interoceptive system that processes body signal differently, and alexithymia is what you call it when the interoceptive deficit specifically interferes with the signal-to-language step.
This is why what’s happening in your body? is a better starting question than what are you feeling? — for any neurodivergent person, and especially for the alexithymic ones. The first question has a possible answer. The second often doesn’t.
What this changes about how you’d actually work on it
If alexithymia is downstream of interoception, the work isn’t to feel more. The work is to build the bridge between body signal and language, in that direction.
Body-first interventions — somatic awareness practices, body scans, interoceptive journalling — are not gentle alternatives to the real work. For an interoceptively atypical brain, they are the real work. The order matters: sensation first, context second, label last. Feel the chest tightness. Notice what was happening when it started. Then, only then, reach for a word, and accept that the word might be approximate, or wrong, or absent. The bridge is being built each time.
This is also why a lot of standard advice falls flat for neurodivergent alexithymics. Emotion wheels and feeling-word lists assume a felt sense already in place; they help the person who knows they are something but not sure what and just needs more vocabulary. They don’t help the person who isn’t getting the signal in the first place. Traditional CBT can run aground for the same reason. The full how-to lives in the living-with-alexithymia guide.
Should you get tested for alexithymia, autism, or ADHD?
Order matters, and cost matters. Alexithymia screening is the cheapest data you can get on yourself — the TAS-20, the Perth Alexithymia Questionnaire, and the OAQ-G2 are all available without a clinician, take 10–15 minutes each, and produce a numerical score that’s actually informative. The test guide walks through which to take and what the scores mean.
Autism and ADHD assessment requires a clinician — usually a psychologist or psychiatrist with relevant experience, often a wait, often a fee, and in some health systems a multi-stage process. Worth doing if the diagnosis would change your access to support, your self-understanding, or your treatment. A high TAS-20 score does not rule autism or ADHD in or out. It just names one of the traits at play. Take the cheapest test first; use what you learn to decide whether the more expensive ones are worth pursuing.
FAQ
Is alexithymia a symptom of autism?
No. Alexithymia is a separate trait that co-occurs with autism at unusually high rates — roughly 50–85% of autistic adults — but it is not a defining feature of autism, and many autistic people do not have it. Bird and Cook’s 2013 alexithymia hypothesis suggests that several emotional features once attributed to autism are better explained by alexithymia. The two share an underlying interoceptive substrate, which is why they overlap so often, but they are independent traits.
Can you have alexithymia without autism or ADHD?
Yes. Roughly one in ten adults meets the threshold in general-population samples, and most of them are neither autistic nor ADHD. It also occurs at elevated rates in PTSD, eating disorders, depression, and chronic-pain populations, and can develop secondarily after sustained trauma or chronic illness. Neurotypical alexithymia is the largest single group, simply because the neurotypical population is so much bigger.
How is ADHD emotional dysregulation different from alexithymia?
ADHD emotional dysregulation is a too much problem — emotions surge fast, hit hard, and are difficult to modulate. Alexithymia is a not getting through problem — the emotion is happening, but the bridge from body to word is broken. They feel different from the inside: the dysregulated ADHDer can usually tell you exactly what they’re feeling, just not control it; the alexithymic person often cannot tell you at all. They can stack, and in the 22–44% of ADHDers who are also alexithymic, the lived experience is both at once.
What is interoception in plain English?
Interoception is your internal sense of what’s going on in your body — your heartbeat, your breathing, your gut, your temperature, the tightness in your chest, the tension in your jaw. It’s the channel by which the body tells the brain what’s happening. Most current emotion theory treats interoception as the raw material of feeling: without a clean read on the body, the brain has nothing to label as fear, sadness, or excitement. Alexithymia is what you call it when that signal-to-language step doesn’t work cleanly.
Should I get tested for autism if I’m alexithymic?
Possibly, but not automatically. A high alexithymia score does not mean you are autistic — it means one trait you have. If you also recognise yourself in autism’s other features (sensory differences, social-energy patterns, monotropic focus, lifelong sense of being a step out of phase), a clinical autism assessment may be worth pursuing, particularly if a diagnosis would unlock support. If you don’t recognise those other features, the alexithymia is likely standing on its own. Either way, working on the alexithymic trait — the interoception-to-language bridge — does not require an autism diagnosis to begin.
Our Emotional Colourblindness guide is written for the trait itself, regardless of whether autism, ADHD, or neither is part of the picture.