You typed am I alexithymic into Google because someone — a partner, a therapist, a stranger on the internet — used the word and it landed somewhere it shouldn’t have. The blank stare when asked how you feel. The body that knows it’s distressed before any word arrives. The compliment that sounds like a foreign language you almost speak.
You want to know which alexithymia test to take, what your score will mean, and whether it actually tells you anything. This article maps the four most-used instruments side by side: the Toronto Alexithymia Scale (TAS-20), the Perth Alexithymia Questionnaire (PAQ), the Online Alexithymia Questionnaire (OAQ-G2), and the Bermond-Vorst Alexithymia Questionnaire (BVAQ). Four tests, one comparison table, a clear recommendation at the end.
Before anything else: this guide is informational, not diagnostic. None of these tests diagnose alexithymia. They screen. A clinician interprets a score; the score doesn’t interpret itself. If you want the longer-form picture of what alexithymia is and isn’t, the pillar essay on alexithymia as a trait, not a disorder is the place to start.
What an alexithymia test actually measures (and what it doesn’t)
Alexithymia is not a feeling-less life. It’s a difficulty naming what’s happening inside you, and the externally-oriented thinking that fills the silence where introspection might otherwise sit. Roughly one in ten adults score in the alexithymic range. The figure rises to between 50% and 85% of autistic adults and around 30-44% of adults with ADHD.
Every credible alexithymia test screens for some combination of three things. Difficulty identifying feelings (DIF): the static where a discrete emotion should be. Difficulty describing feelings (DDF): the gap between knowing something is wrong and being able to say what. Externally-oriented thinking (EOT): a habitual preference for the practical and observable over the inward and emotional. Some tests add fantasy life, sexual function, or interpersonal difficulty; the core triangle is consistent across forty years of research.
What an alexithymia self-assessment does not do: diagnose. None of the four instruments below — not the most-cited TAS-20, not the newest PAQ — were built as diagnostic tools. They were designed to help researchers measure a trait in groups and to help clinicians flag candidates for deeper assessment. A high score is a flag, not a verdict. If a flagged score feels distressing, particularly if you are also navigating depression, trauma, or I don’t feel anything anymore, please talk to someone. Lifeline (Australia) 13 11 14. Samaritans (UK) 116 123. 988 in the US and Canada.
At a glance: comparing the four alexithymia tests
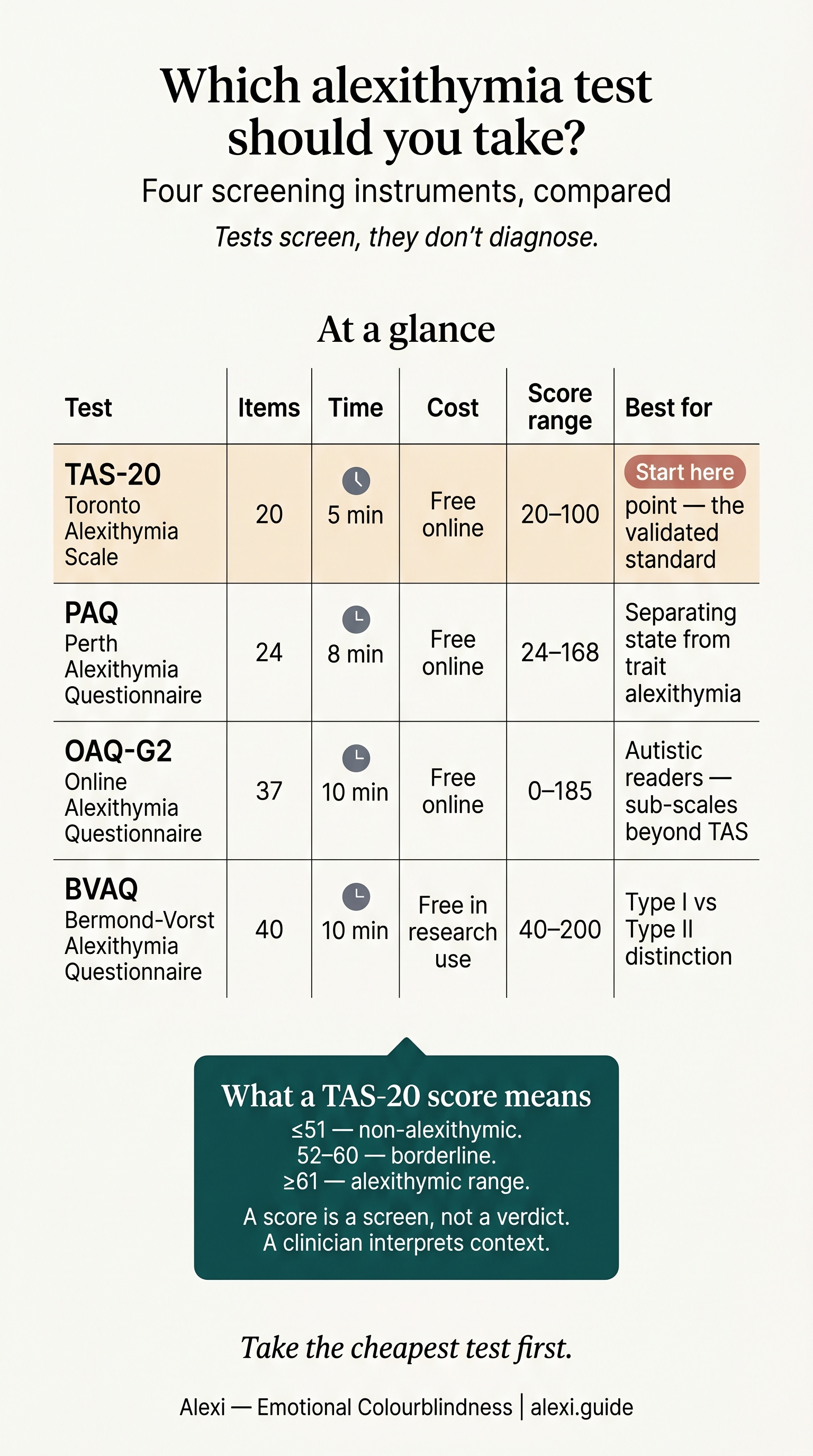
The table below summarises the four instruments most commonly recommended in 2026. Each row is what most readers want to know before they click start.
| Test | Items | Time | Cost | Score range | Sub-factors | Best for |
|---|---|---|---|---|---|---|
| TAS-20 (Toronto Alexithymia Scale) | 20 | 5-10 min | Free online versions widely available | 20-100 (cutoffs: <=51 / 52-60 / >=61) | DIF, DDF, EOT | The default starting point. Fast, validated, internationally normed. |
| PAQ (Perth Alexithymia Questionnaire) | 24 | 7-10 min | Free academic versions; some unofficial online quizzes | Five subscales, no fixed clinical cutoff | N-DIF, P-DIF, N-DDF, P-DDF, G-EOT | Readers who suspect their alexithymia is valence-specific (e.g. blunted on positive emotions). The best-validated measure for autistic adults. |
| OAQ-G2 (Online Alexithymia Questionnaire) | 37 | 7-15 min | Free | 0-185 (0-94 / 95-112 / 113-185) | DIF, DDF, EOT, vicarious interpretation, restricted imagination, interpersonal, sexual | Autistic readers wanting a broader profile, including imagination and interpersonal facets. |
| BVAQ (Bermond-Vorst) | 40 | 10-15 min | Free academic versions on request | 40-200, no universal cutoff | Identifying, Verbalising, Analysing, Fantasising, Emotionalising | Readers who want the Type I vs Type II distinction, particularly if you’re heading into therapy. |
If you only have time for one, take the TAS-20. If you have time for two, take the TAS-20 and the PAQ. The reasoning follows.
1. The Toronto Alexithymia Scale (TAS-20)
If you’ve heard of one alexithymia test, this is it. The TAS-20 was published in 1994 by Michael Bagby, Graeme Taylor, and James Parker as a revision of the earlier 26-item TAS, and it has been the field’s default screening instrument ever since. Translated into more than thirty languages, it is the measure cited in nearly every prevalence study you’ll read.
The structure is unintimidating. Twenty statements, rated 1-5 from strongly disagree to strongly agree. Five items are reverse-scored. Total score runs 20-100 and breaks into three sub-factors: DIF (difficulty identifying feelings, 7 items), DDF (difficulty describing feelings, 5 items), and EOT (externally-oriented thinking, 8 items). The published cutoffs are clean and quotable, which is why every quiz site repeats them:
- 20-51: non-alexithymic.
- 52-60: borderline / possible alexithymia.
- 61-100: alexithymic range.
Strengths. Five to ten minutes. Heavy psychometric backing. Comparable across decades of literature, so a 65 today means roughly what a 65 meant in 1999. Works in clinical and non-clinical samples. The TAS-20 is the closest thing the field has to a common currency.
Limitations. The EOT subscale is the weakest of the three, and translated versions sometimes lose its internal consistency entirely. Several items use abstract or idiomatic phrasing (“I prefer to analyse problems rather than just describe them”) that loads partly on personality style rather than alexithymia. Men score around two points higher than women on average. At least some of that gap is wording bias rather than biology — Levant’s normative male alexithymia literature documents the effect. The single biggest critique is one its own creators acknowledge: people highest in alexithymia may lack the self-awareness needed to answer accurately. The test cannot see itself.
Best for. Anyone starting from zero. Skip if you suspect your difficulty is specifically with positive emotions, or you want a profile broader than the three-factor model.
2. The Perth Alexithymia Questionnaire (PAQ)
The PAQ was published by David Preece and colleagues at Curtin University and Edith Cowan University in 2018, with the definitive 24-item version validated across four samples in 2020. It exists because the TAS-20, for all its dominance, has two limitations the field had been working around for a decade: the EOT subscale’s wobbly cross-cultural validity, and its inability to separate positive-emotion alexithymia from negative-emotion alexithymia.
Twenty-four items, rated on a 7-point Likert scale rather than the TAS-20’s five. Five subscales:
- N-DIF: difficulty identifying negative feelings (sadness, fear, anger).
- P-DIF: difficulty identifying positive feelings (joy, contentment, affection).
- N-DDF: difficulty describing negative feelings.
- P-DDF: difficulty describing positive feelings.
- G-EOT: general externally-oriented thinking.
That valence split is the PAQ’s contribution. A great many people who score in the alexithymic range on the TAS-20 are blunted on one side. The depression-adjacent reader who can describe sadness in detail but goes blank when asked to name good. The trauma-survivor pattern of detailed fear and absent joy. The TAS-20 averages those into a single number; the PAQ doesn’t.
Strengths. Strong psychometrics across cultural samples (Cronbach alpha consistently >= 0.80). The only mainstream alexithymia screening instrument validated specifically with autistic adults — which makes it the current research-community gold standard for that population. A 6-item short form (PAQ-S, 2023) exists for very brief screens.
Limitations. No universally agreed clinical cutoff. The PAQ is interpreted by quartile or by comparing your subscale scores to your own profile, which is statistically defensible but useless if you’re sitting with a number on a screen wondering whether you “are” alexithymic. Free academic copies exist; widely-used online versions are mostly unofficial.
Best for. Readers whose felt sense is I struggle more with one half of the emotional range than the other. Skip if you want a straightforward yes/no number to take to your GP.
3. The Online Alexithymia Questionnaire (OAQ-G2)
If you’ve come to alexithymia through autism — through a partner’s diagnosis, a Reddit thread, an autistic friend — you’ve probably already met the OAQ-G2. It is the autism community’s de facto online alexithymia questionnaire, and it has flaws worth understanding before you cite the result to a clinician.
The OAQ was created by Jason Thompson in 2005 and revised in 2007 (the G2 in OAQ-G2 stands for generation two). Thirty-seven items on a 5-point Likert scale, scored 0-185. Three score bands: 0-94 no alexithymia, 95-112 possible alexithymia, 113-185 alexithymia present. Seven sub-factors, broader than the TAS-20’s three:
- Difficulty identifying feelings.
- Difficulty describing feelings.
- Externally-oriented thinking.
- Vicarious interpretation of feelings — working out what you feel by watching what others feel.
- Restricted imaginative processes.
- Problematic interpersonal relationships.
- Sexual difficulties or disinterest.
That breadth is the OAQ’s selling point. It captures things the TAS-20 doesn’t: the emotional outsourcing, the flat fantasy life, the way alexithymia ripples into intimacy. For autistic readers, the language is more literal and less idiomatic than the TAS-20’s, which removes a known source of measurement error.
Strengths. Free. Subscale-rich. Written for adults whose emotional vocabulary is structurally narrower than neurotypical norms. The autism community trusts it.
Limitations. The OAQ-G2 has never been independently psychometrically validated. It is “based on” validated instruments rather than being one. The seven-factor structure has not been replicated in peer-reviewed work. The interpersonal and sexual subscales risk conflating alexithymia with social-difficulty patterns that have other causes.
Best for. Autistic and AuDHD readers wanting a wider profile than DIF/DDF/EOT alone. Skip if you need a result a clinician will recognise without explanation.
4. The Bermond-Vorst Alexithymia Questionnaire (BVAQ)
The BVAQ is the connoisseur’s option. Published by Harrie Vorst and Bob Bermond at the University of Amsterdam in 2001, it is the only mainstream measure built on the older psychoanalytic model of alexithymia — the one that takes seriously the idea that some alexithymic people genuinely do not feel much, while others feel intensely but cannot process what they feel into thought or speech.
Forty items, five subscales, eight items each:
- Identifying: recognising what you feel.
- Verbalising: putting it into words.
- Analysing: thinking about feelings.
- Fantasising: emotional imagination, daydreaming.
- Emotionalising: the felt intensity of emotional response itself.
Crucially, those five subscales cluster into two higher-order factors — cognitive alexithymia (identifying, verbalising, analysing) and affective alexithymia (fantasising, emotionalising). This is what gives the BVAQ its signature: the Type I / Type II distinction.
- Type I: high on both cognitive and affective measures. The classic “no inner weather” profile — emotion arrives muted or not at all, and what does arrive resists language.
- Type II: high on cognitive measures, normal on affective. Strong emotional life, intact felt intensity, but blocked at the point of identifying or describing it.
The clinical implication matters. Type II tends to respond well to language-based therapies — talk therapy, journalling, emotion-wheel work. Type I usually needs body-first interventions: interoceptive training, somatic experiencing, mindfulness of physical sensation before it gets named. A clinician planning treatment finds this more useful than any single TAS-20 score.
Strengths. Theoretical depth. The only test that maps the Type I/Type II split. Cronbach alpha around 0.79 across subscales.
Limitations. Forty items takes longer than most readers want. No universally agreed clinical cutoff. Free versions exist but typically require a research request rather than a one-click Google find.
Best for. Readers heading into therapy who want their clinician to plan around the result. Skip if you want a five-minute quiz.
The Bottom Line: which alexithymia test should you take?
Take the TAS-20 first. It is free, fast, and the only instrument with cutoffs nearly every clinician will recognise. Score above 60 and you have a number to work with and a literature to read. Score 52-60 and you sit in the borderline range, where a second test will tell you more. Score below 52 and you may not be alexithymic — or you may be alexithymic enough to have under-reported, which is the trait’s central paradox.
Add a second test based on what you noticed while taking the first. If certain items felt strangely easy — naming sadness, naming fear — and others felt impossible — naming joy, naming closeness — take the Perth Alexithymia Questionnaire for its valence split. If you are autistic or strongly suspect you are, take the OAQ-G2 for its broader profile. If you are heading into therapy and want your therapist to plan around your specific shape of alexithymia, take the BVAQ for its Type I/Type II read.
If your score lands in the alexithymic range, the next question is what to do with that — the part nobody Googles for first but everybody needs second. See Living with Alexithymia: a literary, practical guide to building an emotional vocabulary.
FAQ
What’s the most accurate alexithymia test?
The TAS-20 has the strongest psychometric track record across forty years and thirty-plus translations. The PAQ has stronger cross-cultural invariance and is the only measure validated specifically with autistic adults. For most readers in 2026, most accurate means TAS-20 for a single number, PAQ for a more nuanced profile. The OAQ-G2 has not been independently validated; the BVAQ is theoretically richest but rarely used outside research.
Can I diagnose myself with alexithymia using an online test?
No. Alexithymia is not a clinical diagnosis in DSM-5 or ICD-11 — it is a measured trait. Even within research, no test is designed as a diagnostic instrument. Online quizzes screen: they tell you whether your self-reported pattern matches the alexithymic range. A clinician who knows you adds the context the questionnaire cannot capture.
What’s a high TAS-20 score?
A score of 61 or above is considered alexithymic; 52-60 is borderline; 51 or below is non-alexithymic. The scale runs 20-100. Men in non-clinical samples average around 51; women around 49. Scores in the 70s and 80s are unusual but not pathological — alexithymia is a trait, not a severity gauge.
Are alexithymia tests free?
The TAS-20 and the OAQ-G2 are widely available free online. The PAQ is free for academic use, with various unofficial online quizzes inspired by it. The BVAQ is typically free on request from the original researchers. Free does not mean validated — only the TAS-20 and PAQ have peer-reviewed psychometric backing in their official forms.
Should I take more than one alexithymia test?
It is reasonable to. A combined TAS-20 + PAQ takes around fifteen minutes and gives you a robust general score plus a valence-specific profile. Taking the same test twice on different days is also useful — alexithymia varies with state, especially under stress, and a single sitting captures one moment. If two tests agree, the result is more trustworthy than either alone.